How Caffeine Changes Sleep Architecture
TL;DR: Caffeine doesn’t just make it harder to fall asleep. By blocking adenosine signaling, it can reduce slow-wave sleep, increase lighter sleep, fragment the night, and shift REM timing — sometimes without making sleep feel obviously worse.
Your personal caffeine metabolism rate determines whether a morning coffee is cleared by mid-afternoon or means having significant caffeine in your system by bedtime.
Caffeine is usually treated as a timing problem: drink it too late, and you may have trouble falling asleep. That advice is not wrong, but it is incomplete.
The deeper issue is that caffeine interferes with one of the main signals your brain uses to regulate sleep pressure. That signal is adenosine. As adenosine builds across the day, it helps tell the brain that wakefulness has gone on long enough and that sleep should begin. Caffeine blocks that message.
That means caffeine can affect more than sleep onset. When enough caffeine is still active near bedtime, studies show changes in the internal structure of sleep: less slow-wave sleep, more lighter sleep, reduced sleep efficiency, more waking after sleep onset, and context-dependent changes in REM timing (Gardiner et al., 2023; Landolt et al., 1995; Weibel et al., 2021).
The practical trap is that you may not feel the disruption. You can fall asleep, get a normal-looking number of hours, and still have altered sleep architecture under the surface.
This article focuses on the caffeine side of the equation: how caffeine blocks the sleep-pressure system, what it does to sleep architecture, and why the same cutoff time does not work for everyone. For a deeper primer on the sleep stages themselves, see What Sleep Stages Actually Do.
The Short Version: Caffeine Masks Sleep Pressure
Sleep is regulated by two major forces:
- Homeostatic sleep pressure, which builds the longer you are awake.
- Circadian timing, which follows a roughly 24-hour rhythm and helps determine when your brain is biologically prepared for sleep or wakefulness.
Caffeine mainly interferes with the first one.
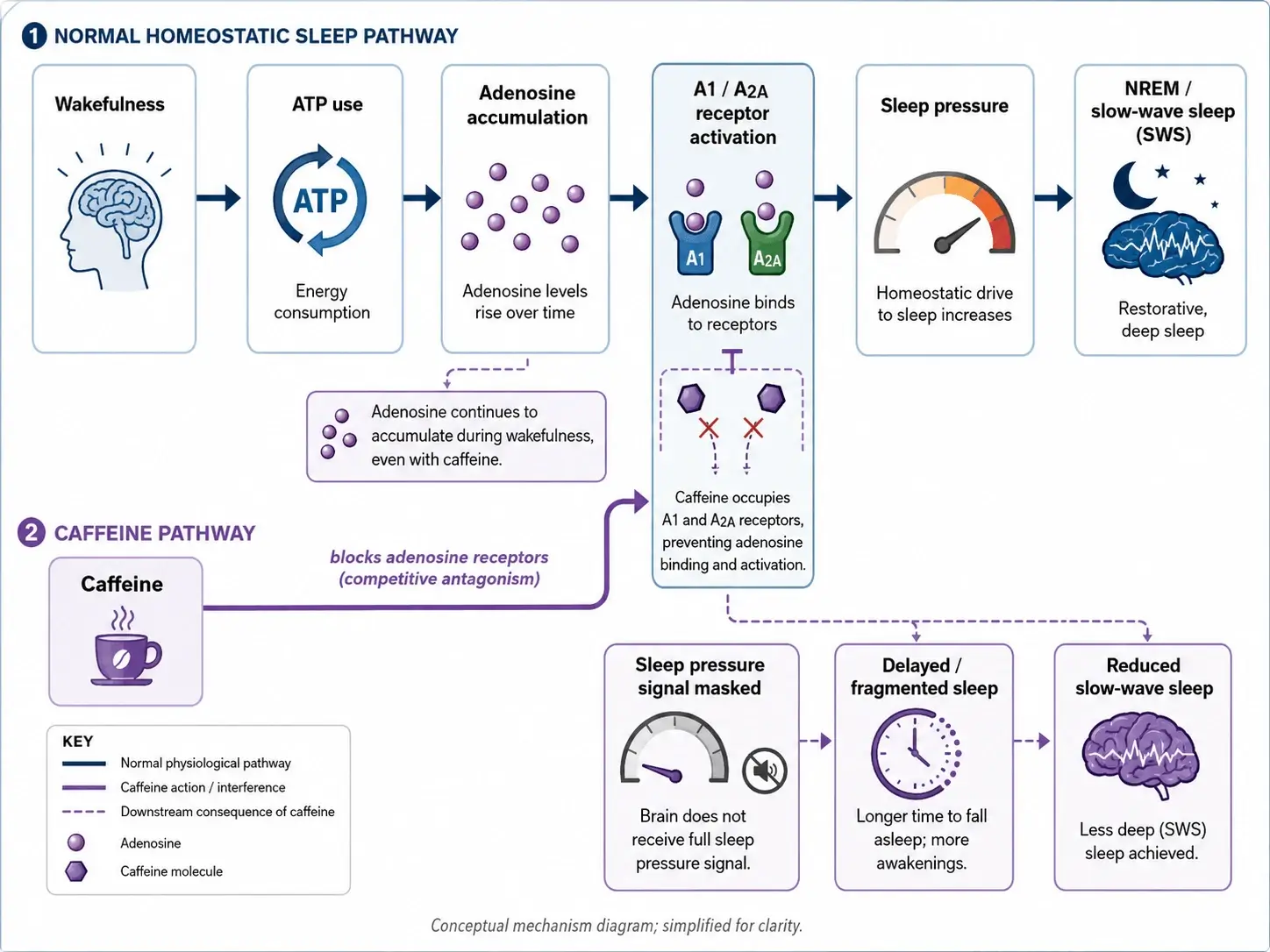
During wakefulness, neurons use energy. As ATP is broken down, adenosine accumulates. Over the day, rising adenosine helps increase sleep pressure by binding to adenosine receptors, especially A1 and A2A receptors. Caffeine is structurally similar enough to adenosine that it can occupy those receptors, but it does not activate them the same way. It sits in the binding site and blocks adenosine from sending the signal.
So caffeine does not erase sleep debt. It masks the readout.
Adenosine keeps accumulating while caffeine is active. Your brain is still building pressure for sleep, but the receptors that would normally detect that pressure are partially blocked. Once caffeine clears, the underlying sleep pressure can become obvious again — the familiar caffeine crash.
What Caffeine Actually Does to Sleep
When meaningful caffeine concentrations are still present at sleep onset, polysomnographic studies — lab-based sleep recordings using EEG and other measures — show a consistent pattern. A 2023 systematic review and meta-analysis of 24 controlled studies found that caffeine reduced total sleep time, reduced sleep efficiency, increased sleep latency, increased wake after sleep onset, increased N1 sleep, and reduced N3 sleep (Gardiner et al., 2023).

Those averages do not mean everyone responds the same way. They do show the broad pattern: caffeine tends to make sleep shorter, lighter, and more fragmented, with a particularly important effect on slow-wave sleep.
Sleep Onset Is Delayed
Caffeine increases sleep latency — the time it takes to fall asleep. In the 2023 meta-analysis, caffeine increased sleep latency by about 9 minutes on average (Gardiner et al., 2023). A 100 mg dose at bedtime has been shown to prolong sleep latency in controlled settings (Landolt et al., 1995), and a randomized crossover trial found that 400 mg significantly delayed sleep initiation when consumed within 12 hours of bedtime (C. L. Gardiner et al., 2025).
That last point matters: caffeine timing is not only about the clock. It is about how much caffeine remains in your system when you try to sleep.
Slow-Wave Sleep Is Suppressed
The most important architectural effect is on slow-wave sleep — also called deep sleep or N3. This is the stage dominated by large, slow delta oscillations. It is concentrated in the first half of the night and is strongly tied to sleep pressure.
The 2023 meta-analysis found that caffeine reduced N3 duration by about 11 minutes on average (C. Gardiner et al., 2023). Multiple studies also show reductions in slow-wave activity, meaning the intensity of delta-band activity within deep sleep, not just the number of minutes spent there (Landolt et al., 1995).
This shows that a night can contain some N3 while still having weaker slow-wave activity. In other words, the architecture may look superficially intact, while the intensity of deep sleep is reduced.
Light Sleep Expands
Where deep sleep is suppressed, lighter sleep often expands. The same meta-analysis found that caffeine increased N1 duration by about 6 minutes and increased the proportion of sleep spent in N1 (C. Gardiner et al., 2023).
N1 is the lightest and most transitional stage of sleep. Replacing N3 with N1 is not a neutral rearrangement. It shifts the night away from deeper, more stable sleep and toward a more wake-adjacent state.
Sleep Gets Shorter and More Fragmented
Caffeine does not just make sleep shorter. It makes it choppier.
Some brief arousals during sleep are normal. What matters is when their frequency, duration, or timing becomes disruptive enough to fragment sleep architecture and interfere with deeper or later-stage sleep.
Across the 24 studies in the meta-analysis, caffeine reduced total sleep time by about 45 minutes and sleep efficiency by 7 percentage points (C. Gardiner et al., 2023). Sleep efficiency is the percentage of time in bed that you are actually asleep. For someone in bed for eight hours, a 7-point drop means roughly 34 more minutes spent awake or drifting in and out of sleep.
Caffeine also increased wake after sleep onset by about 12 minutes (C. Gardiner et al., 2023). That captures time spent awake after first falling asleep, but it does not fully capture brief arousals that may not be remembered the next morning.
Fragmentation matters because sleep is not just a pile of interchangeable minutes. Early cycles are normally rich in slow-wave sleep, while later cycles shift toward longer REM episodes. If caffeine cuts into early deep sleep or replaces it with lighter sleep, the brain does not simply rerun the missed first cycle later. The night continues moving through its normal timing pattern.

Sleep Spindles May Increase
Caffeine does not only reduce deep sleep. It can also reshape the EEG pattern within sleep.
In studies that show reduced low-frequency delta activity, spindle-frequency activity may increase (Landolt et al., 1995). That does not mean caffeine improves sleep. It means the sleeping brain is being pushed into a different electrophysiological pattern than it would naturally produce under high sleep pressure.
REM Effects Are More Variable
Acute caffeine studies show mixed effects on total REM duration. In the 2023 meta-analysis, caffeine did not significantly reduce REM time overall (C. Gardiner et al., 2023).
But regular caffeine use may still affect REM timing. In a controlled study of healthy male habitual caffeine consumers, 10 days of daytime caffeine intake delayed REM sleep promotion and attenuated awakening quality, without clearly reducing total REM percentage across the sleep episode (Weibel et al., 2021).
What does that mean? Caffeine may not reliably reduce total REM time after a single dose, but repeated exposure can still shift when REM occurs, especially under circadian conditions that normally favor REM.
Why Deep Sleep Loss Matters
Slow-wave sleep is not the only important sleep stage. REM and N2 are not side quests. But slow-wave sleep has a special relationship with homeostatic sleep pressure, and that makes it especially vulnerable to caffeine.
N3 and slow-wave activity are tied to several recovery-related processes:
| System | Why slow-wave sleep matters |
|---|---|
| Brain and memory | Supports declarative memory consolidation and synaptic recalibration |
| Hormonal recovery | Coincides with the largest daily pulse of growth hormone secretion |
| Cardiovascular recovery | Helps support the normal nocturnal drop in blood pressure |
| Metabolic regulation | Selective slow-wave sleep suppression can impair insulin sensitivity |
| Brain waste clearance | Provides sleep conditions favorable to glymphatic flow |
The strongest point is not that one lost chunk of N3 causes immediate harm. It is that repeated suppression of slow-wave sleep may matter if it becomes a stable pattern.
Selective slow-wave sleep suppression has been linked to reduced insulin sensitivity (Tasali et al., 2008) and attenuated nocturnal blood pressure dipping (Sayk et al., 2010). Glymphatic clearance also appears most active during NREM slow-wave sleep, meaning caffeine may reduce time spent in the sleep state most favorable to that process.
Why You Might Not Notice
Subjective sleep quality is a poor reporter of sleep architecture.
This is the practical trap. The sleep features most affected by caffeine — especially slow-wave activity in early N3 and subtle fragmentation across the night — are not directly represented in your conscious sense of having slept. You may wake up feeling normal while the architecture of the night was still altered.
In an experimental sleep-fragmentation study, participants had similar total sleep time after fragmented and restorative sleep conditions, but fragmented sleep reduced sleep efficiency, altered N3 and REM, increased fatigue, and impaired inhibition performance (Benkirane et al., 2022). REM disruption is associated with worsened emotional processing, regulation, and learning (Goldstein & Walker, 2014). Repeated arousals (brief awakenings) may also result in weaker overnight motor memory consolidation, even when total sleep time, subjective sleepiness, and other standard sleep measures are similar to normal controls (Djonlagic et al., 2012).
Sleep-related performance changes are not always obvious from the inside. In chronic mild sleep-restriction studies, cognitive performance can decline over days while subjective sleepiness only partially tracks the impairment — indicating people are not always reliable judges of gradual sleep-related cognitive decline (Van Dongen et al., 2003).
This is why “I sleep fine after coffee” is not useless information, but it is incomplete. It tells you whether caffeine obviously disrupted your experience of sleep. It does not tell you whether caffeine changed sleep-stage composition, reduced slow-wave activity, increased subtle fragmentation, or affected the next day’s attention, inhibition, mood regulation, or learning.
Objective measurement is better, but even there, the tool matters. Polysomnography is the gold standard. Validated EEG-based sleep devices can be useful. Consumer wearables can help track trends in sleep duration, timing, awakenings, and consistency, but their sleep-stage estimates should be treated as approximate.
Why Timing Depends on Clearance
Population-level advice like “avoid caffeine after 2 p.m.” is a blunt instrument. The actual question is whether enough caffeine remains at bedtime to interfere with adenosine signaling and slow-wave sleep.
Caffeine half-life varies widely between individuals. CYP1A2, the main liver enzyme responsible for caffeine clearance, is influenced by genetics, smoking, hormonal contraceptives, pregnancy, liver function, and some medications. Sensitivity also varies through adenosine receptor biology, including ADORA2A variation.
That means two people can drink the same amount of caffeine at the same time and reach bedtime with very different caffeine levels.

For someone with a 3-hour half-life, a morning or early-afternoon dose may be mostly cleared by bedtime. For someone with a 8-hour half-life, that same dose can leave a meaningful amount of caffeine active much later.
This is why caffeine guidance should ideally be based on individual clearance, not just average cutoff times.
What the Evidence Supports Most Strongly
| Claim | Evidence strength |
|---|---|
| Caffeine delays sleep onset and reduces total sleep time | Strong |
| Caffeine reduces sleep efficiency and increases wake after sleep onset | Strong |
| Caffeine suppresses N3/SWS and/or slow-wave activity | Strong for acute/evening caffeine |
| Acute caffeine has inconsistent effects on total REM duration | Moderate / mixed |
| Regular caffeine may shift REM timing | Moderate / context-dependent |
| Subjective sleep quality can miss objective architecture changes | Strong |
Practical Implications
A few things follow from this:
-
Timing matters, but clearance is what counts. The relevant variable is not simply when you drank caffeine. It is how much caffeine remains active when your brain is trying to sleep.
-
Deep sleep can be affected even when sleep feels normal. Slow-wave activity can be reduced below conscious detection. Feeling fine is useful information, but it is not the whole signal.
-
The first half of the night is especially important. Slow-wave sleep is concentrated early. Caffeine that delays or fragments the first cycles can affect the portion of sleep most tied to homeostatic recovery.
-
REM effects are not the main acute story. Total REM duration may not reliably drop after a single dose, but REM timing can still shift under some regular-use conditions.
-
Individual variation is the point. Dose, timing, clearance speed, receptor sensitivity, age, tolerance, and baseline sleep quality all affect the outcome.
Bottom Line
Caffeine changes sleep by blocking adenosine receptors, masking the sleep-pressure signal that normally helps drive sleep. That interference can delay sleep onset, reduce total sleep time, increase lighter sleep, fragment the night, and suppress slow-wave sleep or slow-wave activity.
The disruption is not always obvious. You can sleep through the night and still have a different sleep architecture than you would have had without caffeine.
That is why caffeine timing should not be treated as a universal rule. The meaningful question is personal: how much caffeine is still active when your brain is trying to sleep?
References
- Benkirane, O., Delwiche, B., Mairesse, O., & Peigneux, P. (2022). Impact of Sleep Fragmentation on Cognition and Fatigue. Int J Environ Res Public Health, 19(23). https://doi.org/10.3390/ijerph192315485
- Djonlagic, I., Saboisky, J., Carusona, A., Stickgold, R., & Malhotra, A. (2012). Increased sleep fragmentation leads to impaired off-line consolidation of motor memories in humans. PLoS One, 7(3), e34106. https://doi.org/10.1371/journal.pone.0034106
- Gardiner, C. L., Weakley, J., Burke, L. M., Fernandez, F., Johnston, R. D., Leota, J., Russell, S., Munteanu, G., Townshend, A., & Halson, S. L. (2025). Dose and timing effects of caffeine on subsequent sleep: a randomized clinical crossover trial. Sleep, 48(4). https://doi.org/10.1093/sleep/zsae230
- Gardiner, C., Weakley, J., Burke, L. M., Roach, G. D., Sargent, C., Maniar, N., Townshend, A., & Halson, S. L. (2023). The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Medicine Reviews, 69, 101764. https://doi.org/10.1016/j.smrv.2023.101764
- Goldstein, A. N., & Walker, M. P. (2014). The role of sleep in emotional brain function. Annual Review of Clinical Psychology, 10, 679–708. https://doi.org/10.1146/annurev-clinpsy-032813-153716
- Landolt, H. P., Dijk, D. J., Gaus, S. E., & Borbély, A. A. (1995). Caffeine reduces low-frequency delta activity in the human sleep EEG. Neuropsychopharmacology, 12(3), 229–238. https://pubmed.ncbi.nlm.nih.gov/7612156/
- Sayk, F., Teckentrup, C., Becker, C., Heutling, D., Wellhöner, P., Lehnert, H., & Dodt, C. (2010). Effects of selective slow-wave sleep deprivation on nocturnal blood pressure dipping and daytime blood pressure regulation. American Journal of Physiology: Regulatory, Integrative and Comparative Physiology, 298(1), R191–R197. https://doi.org/10.1152/ajpregu.00368.2009
- Tasali, E., Leproult, R., Ehrmann, D. A., & Van Cauter, E. (2008). Slow-wave sleep and the risk of type 2 diabetes in humans. Proceedings of the National Academy of Sciences, 105(3), 1044–1049. https://doi.org/10.1073/pnas.0706446105
- Van Dongen, H. P. A., Maislin, G., Mullington, J. M., & Dinges, D. F. (2003). The Cumulative Cost of Additional Wakefulness: Dose-Response Effects on Neurobehavioral Functions and Sleep Physiology From Chronic Sleep Restriction and Total Sleep Deprivation. Sleep, 26(2), 117–126. https://doi.org/10.1093/sleep/26.2.117
- Weibel, J., Lin, Y.-S., Landolt, H.-P., Berthomier, C., Brandewinder, M., Kistler, J., Rehm, S., Rentsch, K. M., Meyer, M., Borgwardt, S., Cajochen, C., & Reichert, C. F. (2021). Regular Caffeine Intake Delays REM Sleep Promotion and Attenuates Sleep Quality in Healthy Men. J. Biol. Rhythms, 36(4), 384–394. https://doi.org/10.1177/07487304211013995